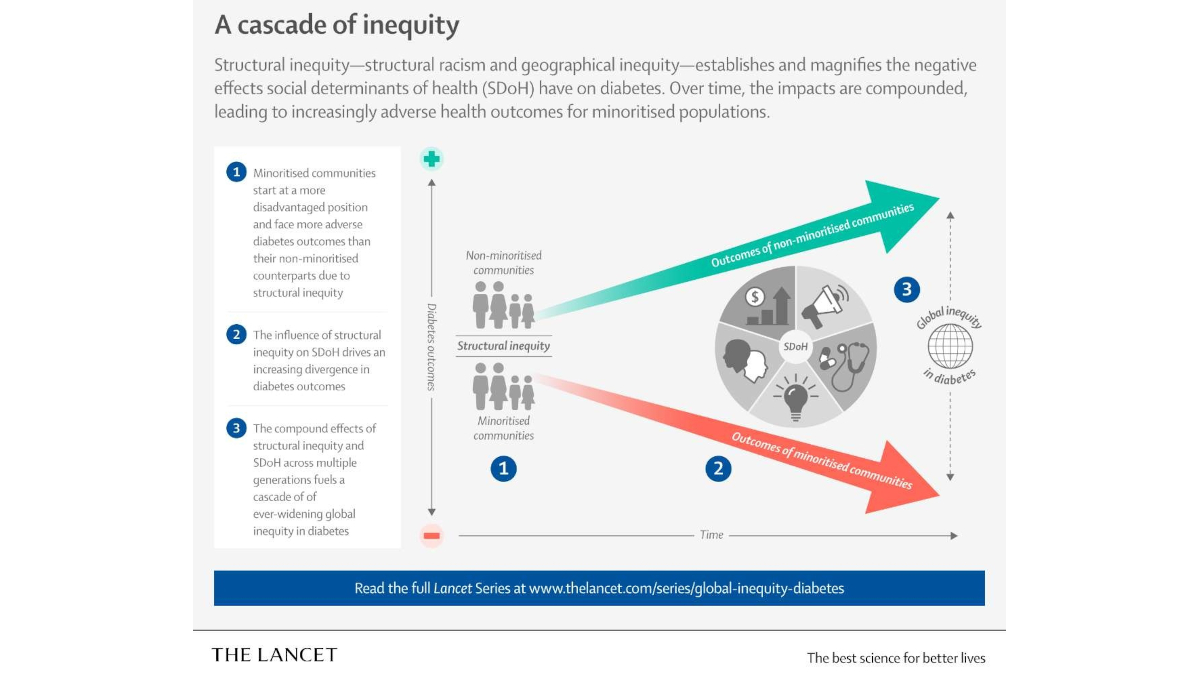
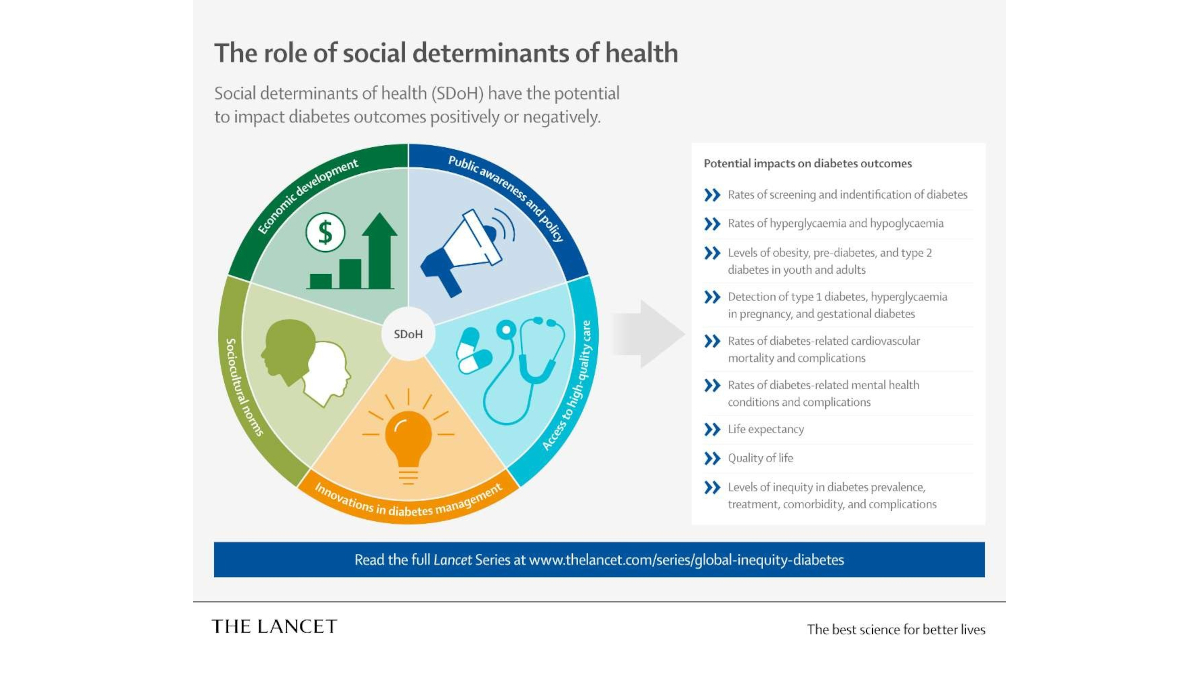
Structural racism and structural conditions in the places where people live and work have far-reaching, transgenerational negative effects on diabetes outcomes across the world. “It is vital that the impact of social and economic factors on diabetes is acknowledged, understood and incorporated into efforts to curb the global diabetes crisis,” said Dr. Agarwal.
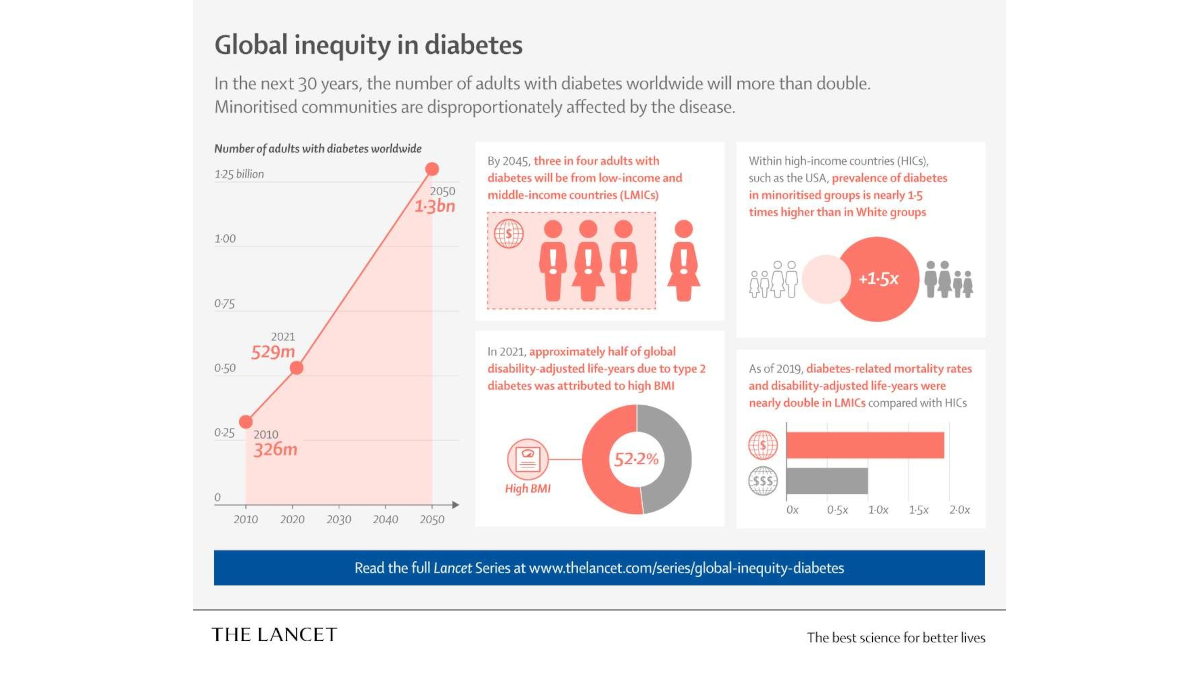
A series article published in The Lancet Diabetes & Endocrinology adds further weight to these findings, highlighting the large disparities in diabetes burden and management that exist between and within race and ethnic groupings in the United States. For example, Black people born in Africa or the Caribbean are 25% less likely to develop diabetes than U.S.-born Black individuals; and Asian, Black and Hispanic individuals and those with low incomes are less likely to receive diabetes treatment with GLP1 receptor agonists than their white or wealthier counterparts.
Opportunities to Improve
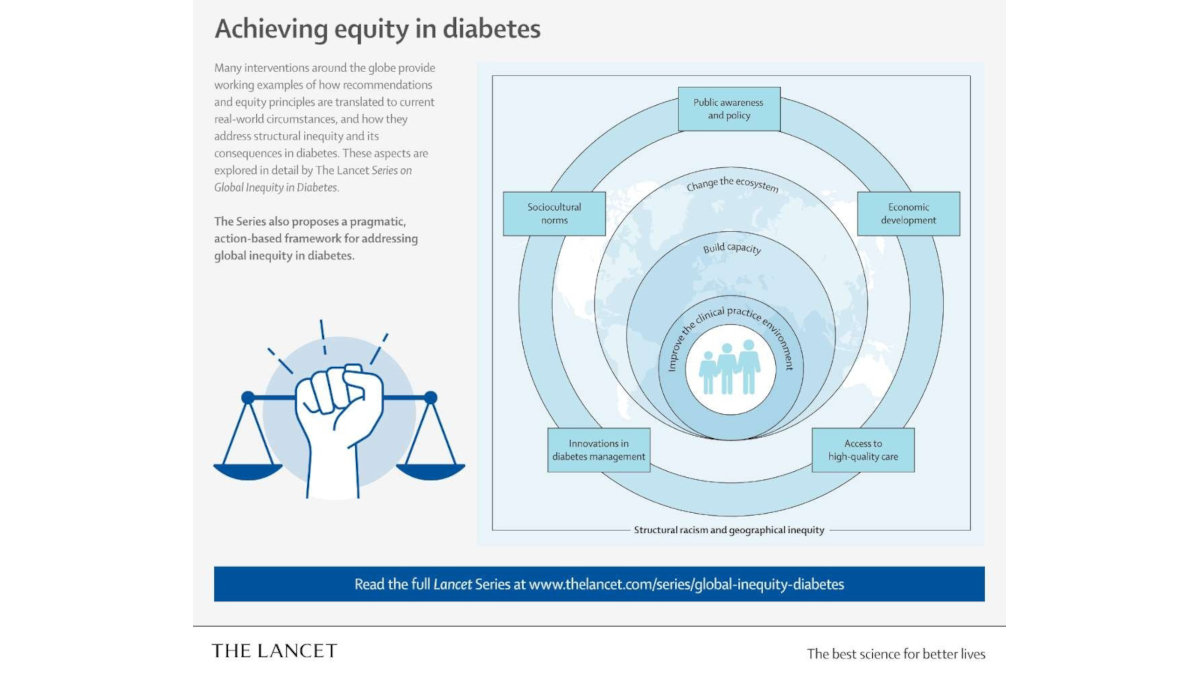
Building on recommendations from The Lancet Commission on diabetes in 2020, together with the 2021 WHO Global Diabetes Compact and the UN Sustainable Development Goals, the series outlines action plans to tackle racial inequities in diabetes care and improve outcomes by including the most affected communities in the development and implementation of interventions and incorporating multilayered strategies to address structural and social determinants of health that are the root causes of inequity globally.
The authors highlight international examples of how to address diabetes inequity in the real world by changing the ecosystem (societal and policy-level factors), building capacity and improving the clinical practice environment.
Insulin access is an important part of the ecosystem for millions of people with diabetes who cannot obtain or afford the necessary supplies to self-manage their diabetes. One intervention in sub-Saharan Africa, developed in partnership with governments, industry and patient groups, is the Diabetes CarePak “co-packaging” solution to increase access to safe insulin and supplies. The month’s supply of test strips, alcohol swabs, needles and syringes and a glucose meter has resulted in more frequent blood glucose monitoring as well as an average hemoglobin A1C decrease of 2.8% over two months—a reduction which compares favorably to medication use.
Ultimately, the series solidifies the need for more high-impact, high-quality, real-world research to ensure that all people with diabetes receive the care they need where and when they need it. “While research has focused on describing these inequities, it is critical to develop and test interventions to address them,” said Dr. Agarwal.